
Treating Arthritis: Making Gains Against The Pain
Although there are 100 types of arthritis, and many forms of treatment, research is getting us close to significant improvements in care. Here are some of the local developments that offer hope.
Arthritis is America’s number one cause of disability, costing the U.S. economy more than $128 billion a year, according to the Arthritis Foundation. The organization’s Southern Arizona Chapter reports that in Arizona alone, approximately 1.1 million people have some form of the disease. Six thousand of those are children.

“Arthritis is a Greek word meaning ‘swelling of the joint,'” says Susan Sweeney, executive director of the Arthritis Foundation’s Greater Southwest Chapter. “Osteoarthritis (OA) is the number one disease in our group; rheumatoid arthritis (RA) is second. Then there’s lupus, which can be of the skin or different kinds; fibromyalgia; or psoriatic arthritis,” the type PGA player Phil Mickelson was diagnosed with in 2010. Autoimmune forms of arthritis have very different causes than OA, but they generally all create joint pain.
Two local medical groups are aggressively pursuing advancements in the field of arthritis, with cutting-edge research being conducted at the Arizona Arthritis Center and innovative patient treatments being done at Tucson Orthopaedic Institute (TOI).
Located on the University of Arizona College of Medicine campus, the Arizona Arthritis Center is headed by Eric Gall, MD, the center’s founder and current interim director.
 He says the main focus at the center is immunology and inflammation. A current study, led by John Szivek, MD, is exploring a new treatment for OA patients. “Dr. Szivek worked with artificial joints early on. Now he’s studying re-growth of cartilage in damaged joints using non-controversial stem cells,” Dr. Gall explains. “They’re taken from the fat of the abdomen, he grows them and reintroduces them to grow into new cartilage. This is a new approach in this area. His lab is waiting to be FDA approved to do the study in humans.”
He says the main focus at the center is immunology and inflammation. A current study, led by John Szivek, MD, is exploring a new treatment for OA patients. “Dr. Szivek worked with artificial joints early on. Now he’s studying re-growth of cartilage in damaged joints using non-controversial stem cells,” Dr. Gall explains. “They’re taken from the fat of the abdomen, he grows them and reintroduces them to grow into new cartilage. This is a new approach in this area. His lab is waiting to be FDA approved to do the study in humans.”
Other research underway at the center includes investigating how to control lupus, clinical studies on pharmaceuticals and a look at valley fever in arthritis patients who are on biologic agents. “Fungal infections can come out in these patients,” and they must go off the drugs, Dr. Gall says. In the past, there’s been uncertainty about whether the patients could continue treatment after valley fever symptoms dissipated. “We’re asking, can you treat again after going off the drug?”
Physicians at Tucson Orthopaedic Institute are attracting attention for three progressive procedures that help those with deteriorating joints. Eric Anctil, MD is performing the Scandinavian Total Ankle Replacement (STAR) surgery, which results in greater range of motion than what’s achieved with other options.
The STAR device, states Dr. Anctil, “is the only implant that’s mobile bearing.” Other ankle replacement devices are fixed bearing and therefore limit motion, as does ankle fusion. The procedure was developed by a Danish surgeon and has been commonplace in Europe and Canada for 15 to 20 years. The Food and Drug Administration approved the technique in the U.S. two years ago.
Anctil moved to Tucson from Canada, where he’d been performing the surgery for years. “When I first came here, I didn’t use another replacement; I waited for the FDA approval. I was the first one in Arizona to do it. Now there are one or two doctors who do the procedure in Tucson and some in Phoenix,” he says.
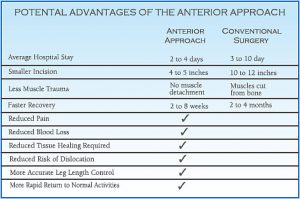
 Those who have put off hip replacement surgery in anticipation of something less invasive now have another option, currently being performed by Edward Petrow Jr., DO. “With anterior hip replacement (AHR), instead of cutting muscle to get to the hip joint, we move the muscle to the side from the front. It’s a quicker initial recovery and patients are off the cane or walker in the first week or two. Other advantages are that there are no hip precautions and a much lower risk for hip dislocation.” The incision, he says, is 8-10 centimeters.
Those who have put off hip replacement surgery in anticipation of something less invasive now have another option, currently being performed by Edward Petrow Jr., DO. “With anterior hip replacement (AHR), instead of cutting muscle to get to the hip joint, we move the muscle to the side from the front. It’s a quicker initial recovery and patients are off the cane or walker in the first week or two. Other advantages are that there are no hip precautions and a much lower risk for hip dislocation.” The incision, he says, is 8-10 centimeters.
Using real time X-ray makes the surgery more precise. “We use the opposite hip as a template to match leg length,” an issue which occasionally arises with other hip replacement techniques, Dr. Petrow notes. AHR is done on a special surgical table that allows extension of the patient’s leg downward, thus giving front access to the hip.
Like Dr. Anctil, Dr. Petrow moved to Tucson from an area where the surgery already was being performed. “I came from Virginia and did it there. I was surprised more people weren’t doing it here.” Dr. Petrow’s primary obstacle was convincing Hospital administrators to purchase the special table at a cost of $70,000 to $120,000, which they eventually did.
 The surgery also requires special training. After performing approximately 40 AHR surgeries during his last year in Virginia and a dozen here, Dr. Petrow believes he’s the most experienced AHR doctor in Tucson. “It’s now sweeping the country,” he adds.
The surgery also requires special training. After performing approximately 40 AHR surgeries during his last year in Virginia and a dozen here, Dr. Petrow believes he’s the most experienced AHR doctor in Tucson. “It’s now sweeping the country,” he adds.
Just approved by the FDA is an innovative procedure for improving ee s, one that uses vitamin E to extend the life of the device. When this article was written, Scott Slagis, MD was the only Tucson doctor lined up to perform the surgery, which will begin once the implants are shipped. He explains that plastics in joint replacements are generally radiated during manufacturing to make them more durable. But radiation releases free radicals into the plastic, which can lead to oxidation and subsequent wear.
“You add vitamin E, which is an antioxidant, and it neutralizes the free radicals. It then may last longer and be stronger,” Dr. Slagis reports. He says the procedure is not age restricted, but it’s especially good for younger, active patients because of its longevity.
Dr. Slagis has seen small advancements in knee replacement procedures, which he’s been performing for 20 years. But he believes the vitamin E implant could prove to be significant. “This is one that may have profound implications,” he says.
Children With Arthritis
Although support programs abound for kids with arthritis, medical attention can be harder to come by, with a shortage of doctors nationwide.
“There are no board-certified pediatric rheumatologists in Southern Arizona, states Deborah Jane Power, DO, of Catalina Pointe Arthritis and Rheumatology Specialists, P.C. “I’m the only rheumatologist in Southern Arizona willing to see kids with juvenile arthritis 15 and younger.” She and her partners also treat adults with RA and OA.
Power explains the differences between the two: “Osteoarthritis is a degenerative, wear-and-tear condition. Some is genetic, some caused by obesity or trauma and bad injuries, such as sports related. The distribution in the body is knees and hips, the base of the thumb and the joint closest to the fingernail.” While she said there are no drugs that slow the progression of OA, taking anti-inflammatory drugs can help, as can exercise.
“Rheumatoid arthritis is an autoimmune disease that starts in the joint. The body attacks the joint lining in the synovial capsule.This causes swelling, pain and loss of range of motion. It’s whole-body inflammation.You also can have fatigue and a low-grade fever,” Power notes.
Nutrition plays a part in arthritis, as well, she says. “Dr. Andrew Weil believes dairy is inflammatory. Things like turmeric, garlic, cayenne and green tea help with inflammation, so patients can be given that. Foods in the nightshade family cause inflammation — tomatoes, potatoes and eggplant.” She suggests that people with RA and other autoimmune diseases avoid gluten, as it can stimulate the immune system.
Arthritis Foundation – Greater Southwest Chapter
The foundation’s primary goals, notes Executive Director Susan Sweeney, are to increase awareness of the disease, raise funds for research and provide local support for people with arthritis. “Money raised in Tucson stays to provide programs and services in Southern Arizona,” she says. These include seminars, health fairs, exercise classes, educational material, referrals, scholarships and kids’ camps — all coordinated out of the Arthritis Foundation’s office at 310 S. Williams Boulevard.
“We have community education classes where a physician and I go out to senior centers, senior communities or to the work place. One big thing we do is arthritis exercise classes. Water exercise and Tai Chi are especially good choices for arthritis patients. We train instructors and have partnerships with Tucson Parks & Recreation, for example.”
Often, it can take eight weeks to see a rheumatologist, according to Sweeney, and people want information on the disease while they wait. “We send them support group information, Arthritis Today magazine and a drug guide from the national office.” Her staff can refer callers to one of eight rheumatology groups in town.
Major fundraising events for the foundation include the Arthritis Walk, held each spring; the Jingle Bell 5K Run & Fun Walk in December; and a newcomer last year, the Surgeons vs. Chefs Pumpkin Carving Contest.
Chris Stead, local Arthritis Walk coordinator, reported that this year’s event drew more than 500 participants and raised approximately $40,000 through pledges, donations and sponsorships. Held at Brandi Fenton Memorial Park on May 7, 2011, the one-mile walk was kicked off by Mayor Bob Walkup, followed by entertainment and activities.
“We had community vendors and booths like Sam’s Club, Desert Diamond Casino and orthopaedic teams,” notes Stead. Ronald McDonald performed magic tricks for the kids, a disc jockey played music and a splash pad cooled everyone Down. “There was a dogathon, and K-9 Loyal Companions gave doggie massages. Dogs get arthritis, too,” Stead remarks.
This year’s holiday-themed 5K fundraiser is slated for Dec. 3 at Reid Park, he says.“It’s a timed run, people dress in holiday gear and we give awards. There’s also a contest with dogs; you can dress up your pet. Funds help with juvenile arthritis family camps and other programs.”
The foundation holds three camps each year: Camp Cruz, a week-long summer camp for 11 to 16 year olds in New Mexico; an overnight camp for younger kids; and a family camp held locally.
As published in Tucson Lifestyle Magazine, December 2011
Written by Christy Krueger
 TUCSON – The first hip replacement surgery was performed in 1960. Now, more than 300,000 total hip replacements are performed each year in the United States.
TUCSON – The first hip replacement surgery was performed in 1960. Now, more than 300,000 total hip replacements are performed each year in the United States.








 As part of the program, the surgeons from Tucson Orthopaedic Institute, and anesthesiologists from Old Pueblo Anesthesia, will donate their time and expertise. Hospitalists will be volunteering time to care for patients after their surgery. Tucson Medical Center is donating the space and necessary prescription medications. Stryker Orthopedics is providing the joints, and Gentiva will provide free home health services to assist these patients during their recovery.
As part of the program, the surgeons from Tucson Orthopaedic Institute, and anesthesiologists from Old Pueblo Anesthesia, will donate their time and expertise. Hospitalists will be volunteering time to care for patients after their surgery. Tucson Medical Center is donating the space and necessary prescription medications. Stryker Orthopedics is providing the joints, and Gentiva will provide free home health services to assist these patients during their recovery.
 Dr. Cohen joined the group this year to help with the mission and to support Dr. Piedrahita’s worthy cause. The team laughed and also cried, and enjoyed each other’s company. The experience left them all feeling enriched and thankful for the chance to give back.
Dr. Cohen joined the group this year to help with the mission and to support Dr. Piedrahita’s worthy cause. The team laughed and also cried, and enjoyed each other’s company. The experience left them all feeling enriched and thankful for the chance to give back.














 Most of us know better than to drain the oil from our car and let the motor run. The heat from the friction would soon cause it to seize, destroying it in minutes.
Most of us know better than to drain the oil from our car and let the motor run. The heat from the friction would soon cause it to seize, destroying it in minutes.
 Dr. Edward Petrow speaks to members of the audience after his talk.
Dr. Edward Petrow speaks to members of the audience after his talk.